
The Ins & Outs of Cholesterol
Cholesterol, what is cholesterol?
I think for most, the first thing that comes to mind when thinking about cholesterol is lipoproteins, or at least their lipid panel, which cholesterol is definitely a part of. Though the various lipoproteins are essentially transport vessels for cholesterol.
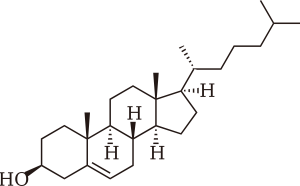
Cholesterol, more specifically, is a waxy fat-like substance produced mainly by the liver and to a lesser extent, the small intestine; otherwise, it is consumed in the diet. It’s a specialized type of lipid structure that has 4 linked hydrocarbons at its core. Essential to cell membrane composition, cholesterol participates in cell fluidity while providing it with structural stability. These structures are also required in hormone production; while the gonads synthesize estrogens and androgens from cholesterol, the adrenals synthesize cortisol and aldosterone, and the skin cholecalciferol [1].
The former may be wonderful and all, but the issue lies in dietary habits. All too often people’s eating patterns are askew and largely meat-based, not to mention really processed. Which are major contributors to vascular conditions as meat and saturated fat (oil) form high amounts of what is known as “bad cholesterol” or low-density lipoproteins (LDLs) [2].

In cholesterol balance, saturated fats (unlike unsaturated fats) have the propensity to reduce the number of LDL receptors in the liver. Which results in an exponential increase in blood and serum concentrations of cholesterol [3]. This is of concern as the LDL makeup has a tendency to collect along the arterial wall and settle in joints where they’re subject to free radical exposure, oxidation, and ultimately inflammation [1].
Which are the key components of atherosclerosis and the progressive state of degradation to the arteries and organs in which the innermost layer or endothelium gradually accumulates bad cholesterol, narrows, and hardens [4]. Arteriosclerosis from the Greek word artéria relating to ‘artery’ and skléros to hard [5]. Disconcerting to say the least as both high cholesterol and hard arteries contribute to a whole slew of problems, most notably HBP, heart attack, stroke, peripheral artery disease, even Alzheimer’s [1].
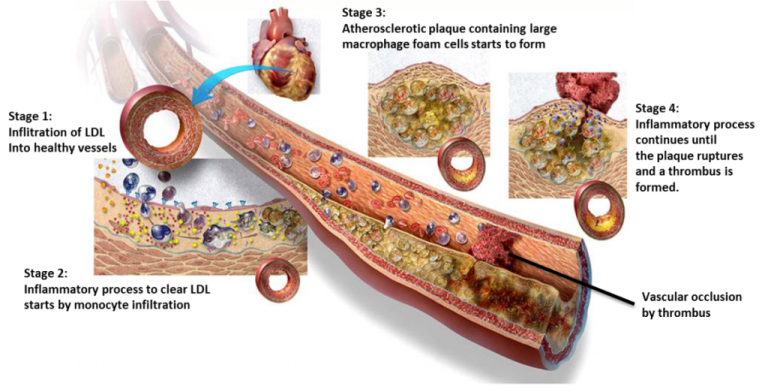
Progressively, as the LDLs undergo oxidation, they initiate an immune response causing white blood cells to either isolate or remove the offending substance. As they become engorged, they take on an appearance of foam. In a perpetual cycle, as these foam cells accumulate more LDLs and die, they create a buildup that ultimately obstructs blood flow. Eventually, muscle cells step in to form a cap and contain the issue, further narrowing the artery. However, if the cap ruptures, the tissue will clot, forming a thrombus that can be life-threatening [4].
When narrowing of the arteries goes unchecked, severe obstructions and blockages have the likelihood to starve tissues and organs of oxygen. For example, narrowing of the tiny vessels within the heart may cause shortness of breath, angina, heart attack, and even heart failure. While narrowing of the carotid (neck artery) starves the brain of oxygen (& nutrients), potentially causing fatigue, headache, gradual hair loss, dizziness, transient attack, or even worse, full-blown stroke (brain damage) [1, 6].

Examples of LDL inducers include red meats such as steaks, ground beef, corned beef, etc., as well as bacon, hot dogs, sausages, and others. Including deli products similar to that of pepperoni, salami, pastrami, etc. Let’s not forget all the fried stuff like shrimp, fish, chips, etc., and to a lesser extent, white meats like poultry with the skin on.
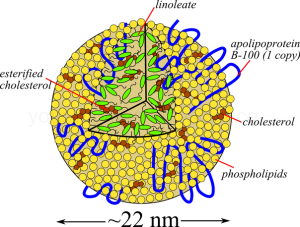
When it comes to modern medicine, cholesterol levels are interpreted through what is known as a “lipid panel,” which measures lipoproteins. Serving as transport vessels of cholesterol (think “total cholesterol”), lipoproteins are molecules with a lipid (cholesterol and triglyceride) core encased by a figurative wetsuit referred to as apolipoprotein [4].
Apolipoproteins facilitate the movement of lipids in blood, lymph, and spinal fluid [4]. As lipids are insoluble in water, the apolipoprotein’s soap-like properties are able to hold and stabilize the said lipids for transport throughout the body [1].
It has been postulated that some individuals with a particular subset of these carrier apolipoprotein vessels (ApoE) involved with LDL’s at receptor sites (LDLR) are implicated in cognitive decline such as Alzheimer’s. Click for a brief overview.
4 specific lipoproteins or types of cholesterol are measured:
● Chylomicrons (CMs) are large, super low in density and move triglycerides to the liver, muscle (such as the heart) & adipose tissue.
● Very Low Density Lipoproteins (VLDLs) are also high in triglycerides but with a higher concentration of “bad cholesterol” and are generally associated with overeating, insulin resistance, & alcohol consumption.
● Intermediate Density Lipoproteins (IDLs), being intermediate are bystanders.
● Low Density Lipoproteins (LDL) aka ‘Bad Cholesterol’ are primarily associated to arterial calcification aka atherosclerosis a leading contributor of cardiovascular disease.
● High Density Lipoproteins (HDLs) are the smallest and most complex of the five groups, aka ‘Good Cholesterol.
Reading The Lipid Panel;
● Total cholesterol = the sum of HDL, LDL, & 20% triglycerides: Normal; less than 200 mg/dL, Borderline high; 200-239 mg/dL, high; 240 mg/dL & above – ie below 200 is the target.
● LDL (Low-Density Lipoprotein) = the bad cholesterol, (ie heart attack, stroke): Optimal; less than 100mg/dL, Borderline high; 130-159 mg/dL, High; 160-189 mg/dL, Extremely high; 190mg/dL – ie 100-129 is the target.
● HDL (High-Density Lipoprotein) = the good cholesterol (decreases risks): Ideal; 60 mg/dL & above, Low (higher risks) less than 40 mg/dL (males), 50 mg/dL (females) – ie above 60 is the target.
● Triglycerides (fat storage for later production of energy) = high LDL in combination with low HDL increases risks (plaque build-up): Normal; less than 150 mg/dL, Borderline high; 150-199 mg/dL, High; 200-499 mg/dL, Extreme high; 500 mg/gL – ie below 150 is the target [7].
Triglycerides, what are triglycerides? You may be wondering.
Triglycerides are a type of mobilized energy reserve serving as intermediates of glucose (sugar) for storage as fat or use in energy formation.
The body’s primary source of energy is glucose, otherwise a simple sugar, and when bodily demand for energy is met, excess dietary sugars (& proteins) get converted into triglycerides for storage as fat. Conversely, in the absence of dietary demands for energy, the body will then mobilize triglycerides from fat for energy formation. ‘Tri-glyceride’ in that it has a 3-carbon sugar alcohol that originated from glucose [1].
Speaking of sugar, let’s talk ‘carbs,’ short for carbohydrate.
Primarily consumed through diet, carbohydrates are chains of sugar molecules. The simplest may be referred to as monosaccharides (glucose, galactose, fructose, etc.) and disaccharides (sucrose, lactose, maltose, etc.) [1].
Regularly refined, concentrated, and put into all kinds of food. These processed sugars are labeled as “added sugars” and are considered “empty calories” as they carry close to no nutritional value.
These simple carbs, aka added sugars, are regularly hidden in surprising places, for example, most meat products, salad dressings, marinara sauce, nutrition bars (energy bars, health bars), delivery & take out, fast food, amongst many others. I assume this is done as a way of getting the consumer to purchase more of the product, as sweet may be euphoric and addicting.
With singular sugars like the monosaccharides, glucose, galactose, & fructose, or the short-chained disaccharides, sucrose, lactose, & maltose, there tends to be a quick breakdown [1].
Click for a brief overview of carbohydrates, check out H.R.’s
With this quick breakdown comes a fast spike in blood sugar, similar to that of throwing gasoline on a fire. As a fire like the blood that blazes with the gas, the flame or energy tends to dwindle just as quickly. Many inflammatory and degenerative conditions are linked with this action.
Ultimately, if those empty calories are not used completely, they get converted to triglycerides and packaged into VLDLs. In fact, no matter the nutritional value, any calories consumed that are not used to the fullest extent and rather quickly will get converted to triglycerides, a collective contributor of high cholesterol.
All of that we’ve discussed has a rather acidic fallout! Let’s call it nutritional ketosis, where there’s a subclinical acidic environment. In relation to ketosis, to quote Atkins, “HIGH PROTEIN DIETS COULD BE AS BAD AS SMOKING”!
Keto, short for ketogenic or ketosis, ultimately relates to a state of high acid (low pH) within the body [8]. Which really alters mucosal biofilms, but that’s a different discussion.
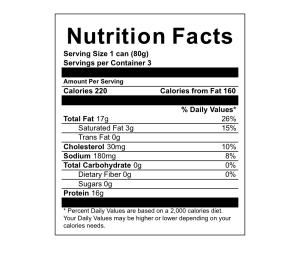
Taking the time to read the “Nutrition Facts Label”, including the ingredients, is helpful. Identify “serving size” while looking out for “saturated fats”, “total cholesterol” (irritability & heartburn indicators), high “sodium” (HBP indicator), “added sugars” (arthritic indicators), and “ingredients” that have additives which are unfamiliar, difficult to pronounce, high in preservatives, or dyes. Goes a long way in reducing total cholesterol, not to mention oxidation and inflammation
Please understand that typically the cascading order in which the ingredients are laid out signifies concentration levels. This goes for meat labels as well, as they also often have “added sugars,” preservatives, and dyes. Including excessive hormones, and antibiotics.
The body uses cholesterol to make bile in an attempt to reduce (acting as an emulsifier) dietary fats ie. cholesterol consumed, for transportation, assimilation, and excretion [1]. Cholesterol comes from the Greek words kholé, relating to ‘bile’, and stereós, to “stiff” [9].
This type of reduction, coupled with the acidic nature of lipids, forms what traditional medicine calls “biliousness,” which correlates with conditions such as GERD (ie heart burn), arthritis (mobility issues), dysbiosis (flatulence, UTI), interstitial cystitis (bladder pain), irritability, and the like [10].
I try to get people to think of bile as a type of solvent. A solvent that the body produces to break down substances that enter it and, depending on what has entered the body, dictates the strength and quantity of bile produced.
Telltale signs of which foods are contributing to high cholesterol usually manifest in symptoms of upper right abdominal discomfort, bloating, or heartburn that occur after consuming (or even thinking about) certain foods. When this happens, the body is essentially pleading for help, indicating that the food was too harmful to be consumed and should be avoided in the future.
Recalling from earlier in our discussion, those saturated fats tend to lower LDL receptors in the liver. Which exponentially increases cholesterol levels within the blood vessels. Well, the indigestion is the body saying, “We’ve got plenty.”
See those LDL receptors of the liver that remove LDL structures from the bloodstream, lowering LDL concentrations overall [3]. The liver breaks down the lipoproteins to free its cholesterol for use in bile production, cell composition, hormone synthesis, vitamin conversion & uptake, fat absorption, & excretion [1]. Clearly, cholesterol is essential; it’s the type of cholesterol that is relevant. The solution to the former is in those high-density lipoproteins or HDLs.
As saturated fats (oils) typically associate with animal products and processed foods, unsaturated oils (fats) associate with fish and plants. Unsaturated oils (fats) induce HDL formation while actually increasing and heightening LDL receptors, ultimately reducing total cholesterol, including triglycerides [3].
Unsaturated oils (fats) not only enhance LDL receptivity of the liver but also participate in Reverse Cholesterol Transport (RCT). In RCT, HDLs actively adhere to LDLs’ structures [4]. HDLs are the smallest, most complex lipoproteins; they actively grab, carry, and remove “bad cholesterol” from arterial walls, thereby reducing bad cholesterol levels, preserving, and even restoring vascular integrity [4].
Examples of HDL inducers include fish and seafood, most nuts, seeds, and beans. As well as olives, avocados, kiwi, etc., pretty much all non-tropical plant-based fats and oils.

Furthermore, plants also produce cholesterol-like structures. Though their attached components differ, these specialized lipid molecules go by the name “Phytosterols” [1]. Within plants, phytosterols serve similar functions as cholesterol does for people. Participating in cell membrane composition and hormone production, yes, plants have hormones; plant sterols are considered to be hormonal messengers serving in plant growth, development, and defense [1].
Being that they closely resemble each other, they compete for absorption in the digestive system, and since plant sterols have a stronger binding affinity, less cholesterol is absorbed [1].
See, while about 50% of dietary cholesterol gets absorbed, only 5% of phytosterols get absorbed (11), and what does get absorbed participates in RCT [4]. Though ubiquitous throughout the plant kingdom, particularly in seeds and grains, heavier concentrations of plant sterols may be found in legumes such as soybeans and peas for example [1].

Moreover, plants (fruits, vegetables, spices, and other herbs) are rich in nutrients and contain what is known as Complex Carbohydrates [2]. Complex carbs are essentially composed of the same sugar molecules as the simple carbs; the difference lays in their formation. As simple carbs contain only one or two sugar molecules, complex carbs contain numerous sugar molecules that come together to form extensively complex structures referred to as polysaccharides [1].
Complex carbohydrates, unlike simple carbs, don’t break down in the same manner. They’ll either be soluble and form gels, or insoluble and serve as “roughage”. Essentially fiber, some polysaccharides contain thousands of joined sugar molecules [1].
When it comes to cholesterol management, gels exhibit multifaceted medicinal actions. Most notably, their binding affinity for bile inhibits its reabsorption, thereby influencing the liver’s utilization of excess cholesterol for further bile production [12]. Furthermore, their coating properties form a protective barrier that reduces fat absorption overall [1].
As for the “roughage”, though to a much lesser extent, also binds with bile, thus reducing its reabsorption, while also supporting satiety. Not only that, but all the phytonutrients plants contain serve various physiological functions.
Side note; the commonly prescribed “Bile Acids Sequestrants” adjuncts regularly prescribed alongside “statins”. To my understanding, work in the same manner as fiber [12]. Though the “Bile Acids Sequestrants” have been associated with a number of gastric complaints. The commonly prescribed “Statins”, to my understanding, inhibit a liver enzyme involved with cholesterol production, decreasing the risk of death after a heart attack. Though they too have been associated with a number of complications [13].
Back to the point, mushrooms are a great example as they’re completely complex, rich in vitamins including D, contain complete protein, and are full of antioxidants [1].

As mentioned earlier, it’s always a good idea to read nutrition labels, so make sure to reserve time during shopping to do so. By choosing foods like seeds, nuts, grains, leafy greens, including brightly colored fruits, and avoiding dietary culprits such as red meat, dairy, simple sugars, and other processed products, a person can effectively lower their high cholesterol levels.
With that, I hope I’ve brought some understanding behind cholesterol. While some risk factors for high cholesterol, like age and family history, may be beyond our control, others, such as diet and lifestyle, can certainly be reduced.
Following are some dietary suggestions to further reduce cholesterol accumulation.
Substitution examples:
● Water with meals over soda or milk.
● Nuts or grains over tater chips.
● Oil & Vinegar over salad dressings.
Plant Powerhouses that protect against high cholesterol:
● Legumes (peas, beans, lentils etc.)
● Brassicas (broccoli, Brussels, collards etc.)
● Alliums (garlic, onion, leeks, chive etc.)
● Mints (organino, basil, thyme, sage etc.)
● Bitters (watercrest, endive, radish, radicchio, sugarloaf, artichoke, kale, cabbage, gobo, etc.)
● Antioxidants (carrots, mushrooms, beets, turmeric, etc.)
Dietary avoidance:
● Saturated fat (beef, veal, poultry, dairy, & to a lesser extent tropical-oils such as palm or coconut oil)
should be no more than 7% of the daily calories.
Dietary inclusions:
● 3 servings omega-3 fatty acid fish; Atlantic herring, salmon, tilapia, sardines, anchovies, etc. weekly.
● 5-7 servings of fruit daily.
Schedule
for herbal integration
Brought to you from Herbal Restoration LLC, Written By Herbalist S. Reese. All Rights Reserved © 2026 Herbal Restoration LLC.
[1] Herbal academy (n.d.) Advanced Clinical Herbalism. Retrieved from; course notes.
[2] Joe Cannon, (2014), Nutrition Essentials; 5th edition, a guid for fitness professionals.
[3] Woollett, L. A., Spady, D. K., & Dietschy, J. M. (1992). Saturated and unsaturated fatty acids independently regulate low density lipoprotein receptor activity and production rate. Journal of lipid research, 33(1), 77–88.
[4] Linton MRF, Yancey PG, Davies SS, et al. (updated 2019) The Role of Lipids and Lipoproteins in Atherosclerosis. Retrived from: https://www.ncbi.nlm.nih.gov/books/NBK343489/
[5] Etymonline (2025) Arteriosclerosis: retrieved from; https://www.etymonline.com/word/arteriosclerosis
[6] Garavaglia C. Jan (2010) Medical Examiner.
[7] University of Health (2025) ATP lll Classification of LDL, Total, and HDL Cholesterol (mg/dl): retrieved from; hr.universityhealthsystem.com
[8] Kolb, H., Kempf, K., Röhling, M., et al. (2021). Ketone bodies: from enemy to friend and guardian angel. BMC medicine, 19(1), 313. https://doi.org/10.1186/s12916-021-02185-0
[9] Etymonline (2025) Cholesterol: retrieved from; https://www.etymonline.com/word/cholesterol
[10] Tobin Graeme (2013) Culpeper’s Medicine: Book; ISBN 978-1-84819-121-1
[11] Li, X., Xin, Y., Mo, Y., et al. (2022). The Bioavailability and Biological Activities of Phytosterols as Modulators of Cholesterol Metabolism. Molecules (Basel, Switzerland), 27(2), 523. https://doi.org/10.3390/molecules27020523
[12] Staels B. Fonseca A. V. (2009) Bile Acids and Metabolic Regulation: Mechanisms and clinical responses to bile acid sequestrants. Diabetes Care 1 32 (supl_2): S237-S245. https://doi.org/10.2337/dc09-S355
[13] Ruscica, M., Ferri, N., Banach, M., et al (2023) Side effects of statins: from pathophysiology and epidemiology to diagnostic and therapeutic implications. Cardiovascular research, 118(17), 3288–3304. https://doi.org/10.1093/cvr/cvac020
Disclaimer
These statements have not been evaluated by the Food and Drug Administration. The educational information published on Herbalrestoration.net is purely for general education. Anything contained on Herbalrestoration.net is not intended to constitute, nor should it be construed, that it is medical advice. The publishers make no claims that the educational information displayed is fit for your medical needs. The information is not to be considered complete and should not be relied on to suggest a course of treatment for a particular illness or disease. Herbalrestoration encourages you to talk to your healthcare providers about any and all supplements, dietary and lifestyle adjustments. The information published on Herbalrestoration.net is not conclusive or exhaustive. The compilation of the information disclaims any and all warranties and liabilities related to the use of any of the information obtained from Herbalrestoration.net or its owners, publishers and authors. Herbalrestoration.net may include links to other websites. These links are provided for the users convenience. They do not signify that we endorse the website(s). We have no responsibility for the content of the linked website(s).
The Ins & Outs of Cholesterol
Cholesterol, what is
cholesterol
I think for most, the first thing that comes to mind when thinking about cholesterol is lipoproteins, or at least their lipid panel, which cholesterol is definitely a part of. Though the various lipoproteins are essentially transport vessels for cholesterol.
Cholesterol, more specifically, is a waxy fat-like substance produced mainly by the liver and to a lesser extent, the small intestine; otherwise, it is consumed in the diet. It’s a specialized type of lipid structure that has 4 linked hydrocarbons at its core. Essential to cell membrane composition, cholesterol participates in cell fluidity while providing it with structural stability. These structures are also required in hormone production; while the gonads synthesize estrogens and androgens from cholesterol, the adrenals synthesize cortisol and aldosterone, and the skin cholecalciferol [1].
The former may be wonderful and all, but the issue lies in dietary habits. All too often people’s eating patterns are askew and largely meat-based, not to mention really processed. Which are major contributors to vascular conditions as meat and saturated fat (oil) form high amounts of what is known as “bad cholesterol” or low-density lipoproteins (LDLs) [2].
In cholesterol balance, saturated fats (unlike unsaturated fats) have the propensity to reduce the number of LDL receptors in the liver. Which results in an exponential increase in blood and serum concentrations of cholesterol [3]. This is of concern as the LDL makeup has a tendency to collect along the arterial wall and settle in joints where they’re subject to free radical exposure, oxidation, and ultimately inflammation [1].
Which are the key components of atherosclerosis and the progressive state of degradation to the arteries and organs in which the innermost layer or endothelium gradually accumulates bad cholesterol, narrows, and hardens [4]. Arteriosclerosis from the Greek word artéria relating to ‘artery’ and skléros to hard [5]. Disconcerting to say the least as both high cholesterol and hard arteries contribute to a whole slew of problems, most notably HBP, heart attack, stroke, peripheral artery disease, even Alzheimer’s [1].
Progressively, as the LDLs undergo oxidation, they initiate an immune response causing white blood cells to either isolate or remove the offending substance. As they become engorged, they take on an appearance of foam. In a perpetual cycle, as these foam cells accumulate more LDLs and die, they create a buildup that ultimately obstructs blood flow. Eventually, muscle cells step in to form a cap and contain the issue, further narrowing the artery. However, if the cap ruptures, the tissue will clot, forming a thrombus that can be life-threatening [4].
When narrowing of the arteries goes unchecked, severe obstructions and blockages have the likelihood to starve tissues and organs of oxygen. For example, narrowing of the tiny vessels within the heart may cause shortness of breath, angina, heart attack, and even heart failure. While narrowing of the carotid (neck artery) starves the brain of oxygen (& nutrients), potentially causing fatigue, headache, gradual hair loss, dizziness, transient attack, or even worse, full-blown stroke (brain damage) [1, 6].
Examples of LDL inducers include red meats such as steaks, ground beef, corned beef, etc., as well as bacon, hot dogs, sausages, and others. Including deli products similar to that of pepperoni, salami, pastrami, etc. Let’s not forget all the fried stuff like shrimp, fish, chips, etc., and to a lesser extent, white meats like poultry with the skin on.
When it comes to modern medicine, cholesterol levels are interpreted through what is known as a “lipid panel,” which measures lipoproteins. Serving as transport vessels of cholesterol (think “total cholesterol”), lipoproteins are molecules with a lipid (cholesterol and triglyceride) core encased by a figurative wetsuit referred to as apolipoprotein [4].
Apolipoproteins facilitate the movement of lipids in blood, lymph, and spinal fluid [4]. As lipids are insoluble in water, the apolipoprotein’s soap-like properties are able to hold and stabilize the said lipids for transport throughout the body [1].
It has been postulated that some individuals with a particular subset of these carrier apolipoprotein vessels (ApoE) involved with LDL’s at receptor sites (LDLR) are implicated in cognitive decline such as Alzheimer’s.
The 4 lipoproteins (Cholesterol types) measured:
· Chylomicrons (CMs) are large, super low in density and move triglycerides to the liver, muscle (such as the heart) & adipose tissue.
· Very Low Density Lipoproteins (VLDLs) are also high in triglycerides but with a higher concentration of “bad cholesterol” and are generally associated with overeating, insulin resistance, & alcohol consumption.
· Intermediate Density Lipoproteins (IDLs), being intermediate are bystanders.
· Low Density Lipoproteins (LDL) aka ‘Bad Cholesterol’ are primarily associated to arterial calcification aka atherosclerosis a leading contributor of cardiovascular disease.
· High Density Lipoproteins (HDLs) are the smallest and most complex of the five groups, aka ‘Good Cholesterol.
Reading The Panel;
· Total cholesterol = the sum of HDL, LDL, & 20% triglycerides: Normal; less than 200 mg/dL, Borderline high; 200-239 mg/dL, high; 240 mg/dL & above.
· LDL (Low-Density Lipoprotein) = the bad cholesterol, (ie heart attack, stroke): Optimal; less than 100mg/dL, Borderline high; 130-159 mg/dL, High; 160-189 mg/dL, Extremely high; 190mg/dL.
· HDL (High-Density Lipoprotein) = the good cholesterol (decreases risks): Ideal; 60 mg/dL & above, Low (higher risks) less than 40 mg/dL (males), 50 mg/dL (females).
· Triglycerides (fat storage for later production of energy) = high LDL in combination with low HDL increases risks (plaque build-up): Normal; less than 150 mg/dL, Borderline high; 150-199 mg/dL, High; 200-499 mg/dL, Extreme high; 500 mg/gL [7].
Triglycerides, what are triglycerides? You may be wondering.
Triglycerides are a type of mobilized energy reserve serving as intermediates of glucose (sugar) for storage as fat or use in energy formation.
The body’s primary source of energy is glucose, otherwise a simple sugar, and when bodily demand for energy is met, excess dietary sugars (& proteins) get converted into triglycerides for storage as fat. Conversely, in the absence of dietary demands for energy, the body will then mobilize triglycerides from fat for energy formation. ‘Tri-glyceride’ in that it has a 3-carbon sugar alcohol that originated from glucose [1].
Speaking of sugar, let’s talk ‘carbs,’ short for carbohydrate.
Primarily consumed through diet, carbohydrates are chains of sugar molecules. The simplest may be referred to as monosaccharides (glucose, galactose, fructose, etc.) and disaccharides (sucrose, lactose, maltose, etc.) [1].
Regularly refined, concentrated, and put into all kinds of food. These processed sugars are labeled as “added sugars” and are considered “empty calories” as they carry close to no nutritional value.
These simple carbs, aka added sugars, are regularly hidden in surprising places, for example, most meat products, salad dressings, marinara sauce, nutrition bars (energy bars, health bars), delivery & take out, fast food, amongst many others. I assume this is done as a way of getting the consumer to purchase more of the product, as sweet may be euphoric and addicting.
With singular sugars like the monosaccharides, glucose, galactose, & fructose, or the short-chained disaccharides, sucrose, lactose, & maltose, there tends to be a quick breakdown [1].
With this quick breakdown comes a fast spike in blood sugar, similar to that of throwing gasoline on a fire. As a fire like the blood that blazes with the gas, the flame or energy tends to dwindle just as quickly. Many inflammatory and degenerative conditions are linked with this action.
Curious about carbohydrates, check out H.R.’s Macro-nutrition pg.
Ultimately, if those empty calories are not used completely, they get converted to triglycerides and packaged into VLDLs. In fact, no matter the nutritional value, any calories consumed that are not used to the fullest extent and rather quickly will get converted to triglycerides, a collective contributor of high cholesterol.
All of that we’ve discussed has a rather acidic fallout! Let’s call it nutritional ketosis, where there’s a subclinical acidic environment. In relation to ketosis, to quote Atkins, “HIGH PROTEIN DIETS COULD BE AS BAD AS SMOKING”!
Keto, short for ketogenic or ketosis, ultimately relates to a state of high acid (low pH) within the body [8]. Which really alters mucosal biofilms, but that’s a different discussion.
Taking the time to read the “Nutrition Facts” label, including the ingredients, is helpful. Identify “serving size” while looking out for “saturated fats”, “total cholesterol” (irritability & heartburn indicators), high “sodium” (HBP indicator), “added sugars” (arthritic indicators), and “ingredients” that have additives which are unfamiliar, difficult to pronounce, high in preservatives, or dyes. Goes a long way in reducing total cholesterol, not to mention oxidation and inflammation
Please understand that typically the cascading order in which the ingredients are laid out signifies concentration levels. This goes for meat labels as well, as they also often have “added sugars,” preservatives, and dyes. Including excessive hormones, and antibiotics.
The body uses cholesterol to make bile in an attempt to reduce (acting as an emulsifier) dietary fats ie. cholesterol consumed, for transportation, assimilation, and excretion [1]. Cholesterol comes from the Greek words kholé, relating to ‘bile’, and stereós, to “stiff” [9].
This type of reduction, coupled with the acidic nature of lipids, forms what traditional medicine calls “biliousness,” which correlates with conditions such as GERD (ie heart burn), arthritis (mobility issues), dysbiosis (flatulence, UTI), interstitial cystitis (bladder pain), irritability, and the like [10].
I try to get people to think of bile as a type of solvent. A solvent that the body produces to break down substances that enter it and, depending on what has entered the body, dictates the strength and quantity of bile produced.
Telltale signs of which foods are contributing to high cholesterol usually manifest in symptoms of upper right abdominal discomfort, bloating, or heartburn that occur after consuming (or even thinking about) certain foods. When this happens, the body is essentially pleading for help, indicating that the food was too harmful to be consumed and should be avoided in the future.
Recalling from earlier in our discussion, those saturated fats tend to lower LDL receptors in the liver. Which exponentially increases cholesterol levels within the blood vessels. Well, the indigestion is the body saying, “We’ve got plenty.”
See those LDL receptors of the liver that remove LDL structures from the bloodstream, lowering LDL concentrations overall [3]. The liver breaks down the lipoproteins to free its cholesterol for use in bile production, cell composition, hormone synthesis, vitamin conversion & uptake, fat absorption, & excretion [1]. Clearly, cholesterol is essential; it’s the type of cholesterol that is relevant. The solution to the former is in those high-density lipoproteins or HDLs.
As saturated fats (oils) typically associate with animal products and processed foods, unsaturated oils (fats) associate with fish and plants. Unsaturated oils (fats) induce HDL formation while actually increasing and heightening LDL receptors, ultimately reducing total cholesterol, including triglycerides [3].
Unsaturated oils (fats) not only enhance LDL receptivity of the liver but also participate in Reverse Cholesterol Transport (RCT). In RCT, HDLs actively adhere to LDLs’ structures [4]. HDLs are the smallest, most complex lipoproteins; they actively grab, carry, and remove “bad cholesterol” from arterial walls, thereby reducing bad cholesterol levels, preserving, and even restoring vascular integrity [4].
Examples of HDL inducers include fish and seafood, most nuts, seeds, and beans. As well as olives, avocados, kiwi, etc., pretty much all non-tropical plant-based fats and oils.
Furthermore, plants also produce cholesterol-like structures. Though their attached components differ, these specialized lipid molecules go by the name “Phytosterols” [1]. Within plants, phytosterols serve similar functions as cholesterol does for people. Participating in cell membrane composition and hormone production, yes, plants have hormones; plant sterols are considered to be hormonal messengers serving in plant growth, development, and defense [1].
Being that they closely resemble each other, they compete for absorption in the digestive system, and since plant sterols have a stronger binding affinity, less cholesterol is absorbed [1].
See, while about 50% of dietary cholesterol gets absorbed, only 5% of phytosterols get absorbed (11), and what does get absorbed participates in RCT [4]. Though ubiquitous throughout the plant kingdom, particularly in seeds and grains, heavier concentrations of plant sterols may be found in legumes such as soybeans and peas for example [1].
Moreover, plants (fruits, vegetables, spices, and other herbs) are rich in nutrients and contain what is known as Complex Carbohydrates [2]. Complex carbs are essentially composed of the same sugar molecules as the simple carbs; the difference lays in their formation. As simple carbs contain only one or two sugar molecules, complex carbs contain numerous sugar molecules that come together to form extensively complex structures referred to as polysaccharides [1].
Complex carbohydrates, unlike simple carbs, don’t break down in the same manner. They’ll either be soluble and form gels, or insoluble and serve as “roughage”. Essentially fiber, some polysaccharides contain thousands of joined sugar molecules [1].
When it comes to cholesterol management, gels exhibit multifaceted medicinal actions. Most notably, their binding affinity for bile inhibits its reabsorption, thereby influencing the liver’s utilization of excess cholesterol for further bile production [12]. Furthermore, their coating properties form a protective barrier that reduces fat absorption overall [1].
As for the “roughage”, though to a much lesser extent, also binds with bile, thus reducing its reabsorption, while also supporting satiety. Not only that, but all the phytonutrients plants contain serve various physiological functions.
Side note; the commonly prescribed “Bile Acids Sequestrants” adjuncts regularly prescribed alongside “statins”. To my understanding, work in the same manner as fiber [12]. Though the “Bile Acids Sequestrants” have been associated with a number of gastric complaints. The commonly prescribed “Statins”, to my understanding, inhibit a liver enzyme involved with cholesterol production, decreasing the risk of death after a heart attack. Though they too have been associated with a number of complications [13].
Back to the point, mushrooms are a great example as they’re completely complex, rich in vitamins including D, contain complete protein, and are full of antioxidants [1].
As mentioned earlier, it’s always a good idea to read nutrition labels, so make sure to reserve time during shopping to do so. By choosing foods like seeds, nuts, grains, leafy greens, including brightly colored fruits, and avoiding dietary culprits such as red meat, dairy, simple sugars, and other processed products, a person can effectively lower their high cholesterol levels.
With that, I hope I’ve brought some understanding behind cholesterol. While some risk factors for high cholesterol, like age and family history, may be beyond our control, others, such as diet and lifestyle, can certainly be reduced.
Following are some dietary suggestions to further reduce cholesterol accumulation.
Substitution examples:
· Water with meals over soda or milk.
· Nuts or grains over tater chips.
· Oil & Vinegar over salad dressings.
Plant Powerhouses that protect against high cholesterol:
· Legumes (peas, beans, lentils etc.)
· Brassicas (broccoli, Brussels, collards etc.)
· Alliums (garlic, onion, leeks, chive etc.)
· Mints (organino, basil, thyme, sage etc.)
· Bitters (watercrest, endive, radish, radicchio, sugarloaf, artichoke, kale, cabbage, gobo, etc.)
· Antioxidants (carrots, mushrooms, beets, turmeric, etc.)
Dietary avoidance:
· Saturated fat (beef, veal, poultry, dairy, tropical-oils i.e. palm or coconut oil) should be no more than 7% of the daily calories.
Dietary inclusions:
· 3 servings omega-3 fatty acid fish; Atlantic herring, salmon, tilapia, sardines, anchovies, etc. weekly.
· 5-7 servings of fruit daily.
Brought to you from Herbal Restoration LLC, Written By Herbalist S. Reese. All Rights Reserved © 2026 Herbal Restoration LLC.
[1] Herbal academy (n.d.) Advanced Clinical Herbalism. Retrieved from; course notes.
[2] Joe Cannon, (2014), Nutrition Essentials; 5th edition, a guid for fitness professionals.
[3] Woollett, L. A., Spady, D. K., & Dietschy, J. M. (1992). Saturated and unsaturated fatty acids independently regulate low density lipoprotein receptor activity and production rate. Journal of lipid research, 33(1), 77–88.
[4] Linton MRF, Yancey PG, Davies SS, et al. (updated 2019) The Role of Lipids and Lipoproteins in Atherosclerosis. Retrived from: https://www.ncbi.nlm.nih.gov/books/NBK343489/
[5] Etymonline (2025) Arteriosclerosis: retrieved from; https://www.etymonline.com/word/arteriosclerosis
[6] Garavaglia C. Jan (2010) Medical Examiner.
[7] University of Health (2025) ATP lll Classification of LDL, Total, and HDL Cholesterol (mg/dl): retrieved from; hr.universityhealthsystem.com
[8] Kolb, H., Kempf, K., Röhling, M., et al. (2021). Ketone bodies: from enemy to friend and guardian angel. BMC medicine, 19(1), 313. https://doi.org/10.1186/s12916-021-02185-0
[9] Etymonline (2025) Cholesterol: retrieved from; https://www.etymonline.com/word/cholesterol
[10] Tobin Graeme (2013) Culpeper’s Medicine: Book; ISBN 978-1-84819-121-1
[11] Li, X., Xin, Y., Mo, Y., et al. (2022). The Bioavailability and Biological Activities of Phytosterols as Modulators of Cholesterol Metabolism. Molecules (Basel, Switzerland), 27(2), 523. https://doi.org/10.3390/molecules27020523
[12] Staels B. Fonseca A. V. (2009) Bile Acids and Metabolic Regulation: Mechanisms and clinical responses to bile acid sequestrants. Diabetes Care 1 32 (supl_2): S237-S245. https://doi.org/10.2337/dc09-S355
[13] Ruscica, M., Ferri, N., Banach, M., et al (2023) Side effects of statins: from pathophysiology and epidemiology to diagnostic and therapeutic implications. Cardiovascular research, 118(17), 3288–3304. https://doi.org/10.1093/cvr/cvac020
Disclaimer
These statements have not been evaluated by the Food and Drug Administration. The educational information published on Herbalrestoration.net is purely for general education. Anything contained on Herbalrestoration.net is not intended to constitute, nor should it be construed, that it is medical advice. The publishers make no claims that the educational information displayed is fit for your medical needs. The information is not to be considered complete and should not be relied on to suggest a course of treatment for a particular illness or disease. Herbalrestoration encourages you to talk to your healthcare providers about any and all supplements, dietary and lifestyle adjustments. The information published on Herbalrestoration.net is not conclusive or exhaustive. The compilation of the information disclaims any and all warranties and liabilities related to the use of any of the information obtained from Herbalrestoration.net or its owners, publishers and authors. Herbalrestoration.net may include links to other websites. These links are provided for the users convenience. They do not signify that we endorse the website(s). We have no responsibility for the content of the linked website(s).